
When you wake up one morning and notice your vision is blurry or dark in one eye - no pain, no warning - it can be terrifying. For many, this is the first sign of retinal vein occlusion (RVO), a serious eye condition that blocks the tiny veins carrying blood away from the retina. It doesn’t happen overnight, but it hits fast. And if left untreated, it can lead to permanent vision loss. The good news? We now have effective treatments, especially injections that can save sight. But knowing your risks and what to expect from treatment makes all the difference.
What Exactly Is Retinal Vein Occlusion?
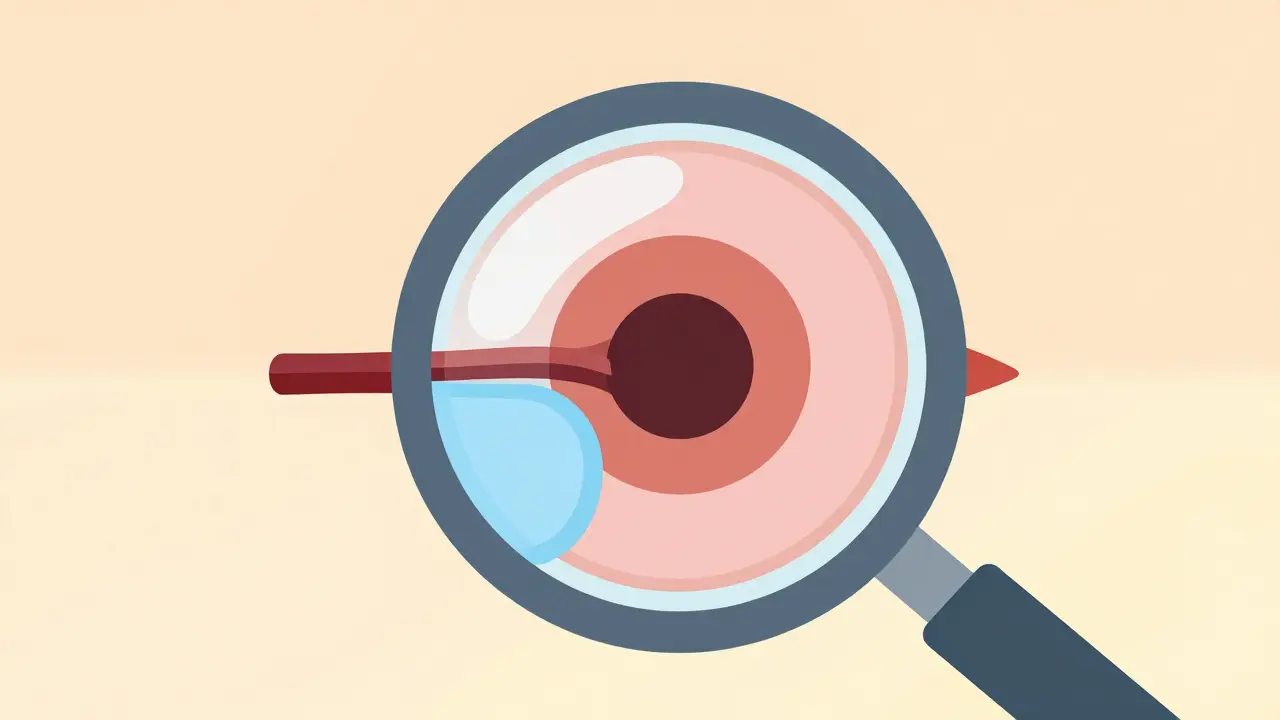
The retina is the light-sensitive layer at the back of your eye. It turns images into signals your brain understands. When a vein in the retina gets blocked, fluid leaks out, swelling the macula - the center part of the retina responsible for sharp, detailed vision. This swelling, called macular edema, is what blurs your vision. There are two main types of RVO:- Central Retinal Vein Occlusion (CRVO): The main vein is blocked. This usually causes more severe vision loss.
- Branch Retinal Vein Occlusion (BRVO): A smaller branch vein is blocked. Vision loss is often partial, affecting just one part of your visual field.
Who’s Most at Risk?
RVO isn’t random. It’s tied to long-term health habits and conditions. Most cases happen after age 55, and over half occur in people over 65. But it’s not just about age.- High blood pressure is the biggest risk factor. Up to 73% of CRVO patients over 50 have uncontrolled hypertension. Even if you think your blood pressure is "okay," consistently high numbers damage blood vessels over time.
- Diabetes affects about 10% of RVO patients over 50. High blood sugar weakens tiny blood vessels, making them more likely to leak or clot.
- High cholesterol (total cholesterol above 6.5 mmol/L) is found in 35% of all RVO cases. Fatty deposits build up in artery walls, increasing pressure and narrowing blood flow.
- Glaucoma and high eye pressure raise the risk, especially if the blockage happens near the optic nerve.
- Smoking is involved in 25-30% of cases. It thickens blood, damages vessel walls, and speeds up hardening of the arteries.
- Obesity and lack of movement contribute. Sedentary lifestyles worsen circulation and increase inflammation.
- Oral contraceptives - especially in women with other risk factors like high blood pressure.
- Blood disorders like polycythemia vera, multiple myeloma, or inherited clotting problems (like factor V Leiden).
How Do Injections Help?
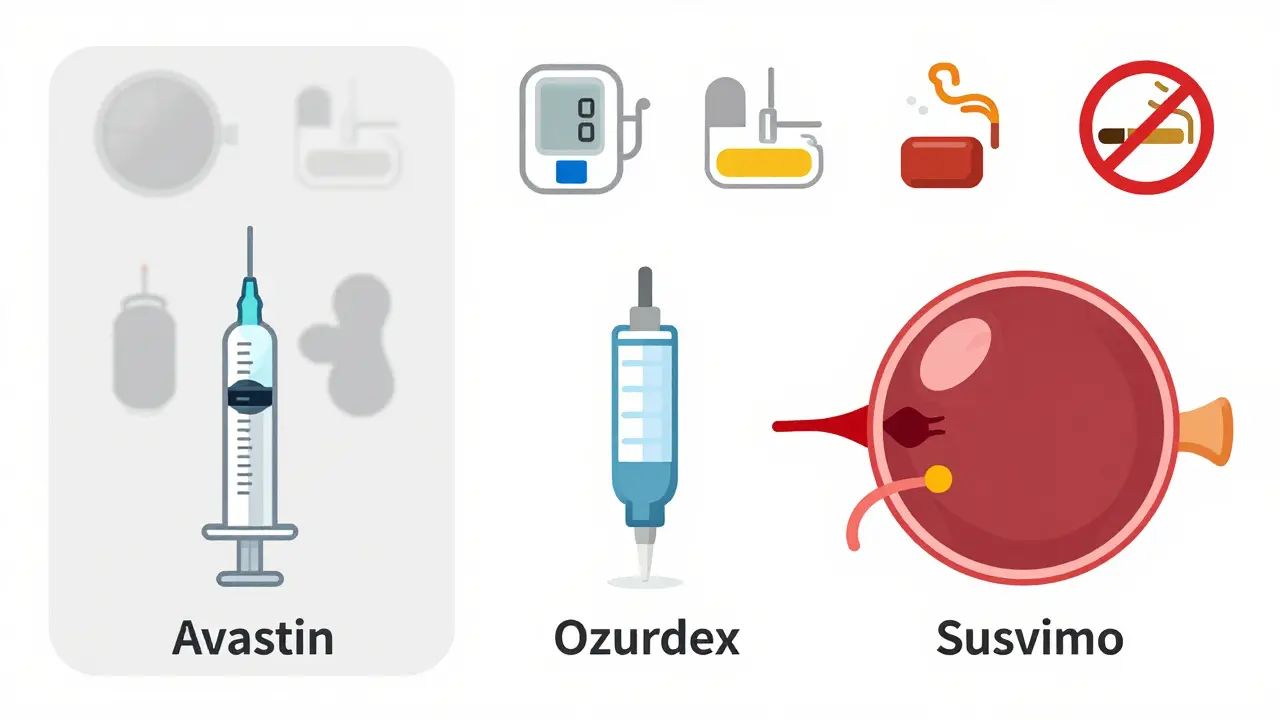
Injections into the eye - yes, really - are now the standard treatment. They don’t fix the blocked vein. Instead, they stop the damage the blockage causes: swelling in the macula. Two types of injections are used:- Anti-VEGF drugs: These block a protein called VEGF that causes fluid leakage. Common ones include ranibizumab (Lucentis), aflibercept (Eylea), and bevacizumab (Avastin - used off-label).
- Corticosteroid implants: Like Ozurdex, a tiny implant that slowly releases steroid into the eye to reduce inflammation.

What to Expect During Treatment
Getting an injection sounds scary, but it’s quick and routine. Here’s what happens:- You’ll get numbing drops in your eye.
- Your eye is cleaned with antiseptic.
- A tiny speculum holds your eyelid open.
- The doctor injects the medicine through the white part of your eye - not the front.
- The whole thing takes 5-7 minutes.
Cost and Real-Life Challenges
This is where things get tough. Anti-VEGF drugs are expensive. In the U.S., Lucentis and Eylea cost around $2,000 per dose. Avastin, which is the same drug but repackaged from cancer treatment, costs about $50. That’s why many safety-net clinics use Avastin - it works just as well. But cost isn’t the only burden. Many patients report:- Financial strain - $150-$2,000 per injection adds up fast.
- Treatment fatigue - going to the clinic every month for over a year is exhausting.
- Anxiety - the fear of needles, even when you know it’s safe.
What’s New in Treatment?
The field is moving fast. New approaches aim to reduce how often you need injections:- Port Delivery System (Susvimo): A tiny refillable implant placed in the eye that releases ranibizumab for months. Approved for AMD, trials for RVO are underway.
- Gene therapy: RGX-314 is being tested to make your eye produce its own anti-VEGF protein - potentially eliminating injections altogether.
- Combination therapy: Some doctors now mix anti-VEGF with steroids for patients who don’t respond to one alone.
What You Can Do
If you’re at risk - or already have RVO - here’s what matters most:- Control your blood pressure. Even small drops in numbers help.
- Manage diabetes and cholesterol. Get regular labs.
- Quit smoking. No exceptions.
- Move daily. A 20-minute walk improves circulation.
- See your eye doctor every 3-6 months if you’ve had RVO. Monitoring with OCT scans catches swelling before it hurts vision.
- Ask about treatment options. Don’t assume one drug is right for everyone.
Can retinal vein occlusion be cured?
No, RVO itself can’t be cured - the blocked vein doesn’t reopen. But the damage it causes - like macular edema - can be controlled. Injections stop fluid buildup, preserve vision, and often improve it. Many patients maintain good vision for years with ongoing treatment.
Are eye injections painful?
Most patients feel pressure or a brief pinch, but not sharp pain. Numbing drops are used, and the procedure takes less than 10 minutes. Some report mild irritation or a scratchy feeling afterward, but it fades within hours.
How long until I see improvement after an injection?
Some patients notice better vision within days. For most, it takes 2-6 weeks. OCT scans track swelling reduction, which is the real sign of progress. Don’t expect instant results - consistent treatment over months is what matters.
Can I get RVO in both eyes?
Yes, but it’s rare. Most cases affect only one eye. If you’ve had RVO in one eye, your risk of it happening in the other increases slightly - especially if underlying conditions like high blood pressure or diabetes aren’t controlled. Regular eye exams are critical.
Is there a difference between Avastin, Lucentis, and Eylea?
All three block VEGF and work similarly. Clinical trials show Eylea and Lucentis have slightly better average results in some cases. But Avastin, which costs 40 times less, is just as effective for most people. The choice often comes down to cost, insurance coverage, and doctor preference.
 Medications
Medications



Milad Jawabra
March 5, 2026 AT 17:26Bro, I had CRVO last year. Didn’t think I’d ever read my kid’s homework again. Got 11 injections in 8 months. Avastin. Cost me $50 a pop thanks to my VA clinic. Vision’s back to 20/30. Not perfect, but I can see faces now. Don’t let fear stop you - this shit works. 🤝
Jessica Chaloux
March 5, 2026 AT 18:48I cried the first time I got the injection. Not because it hurt - because I realized I’d been ignoring my BP for YEARS. My mom died from a stroke. I didn’t want to end up blind too. Now I take my meds. Walk every morning. And yes, I still cry sometimes. 😭
Mariah Carle
March 6, 2026 AT 01:22It’s funny how medicine treats symptoms while ignoring the metaphysical. The retina is a mirror of the soul’s stagnation. A blocked vein? That’s not just a clot - it’s a refusal to flow. We live in a world that commodifies health, turning vision into a subscription service. Eylea costs $2000? Or is it the cost of ignoring your body’s whispers until it screams? 🌌
Megan Nayak
March 7, 2026 AT 03:38Let’s be real - this whole ‘injection miracle’ narrative is corporate propaganda. Anti-VEGF drugs? They’re just Band-Aids on a hemorrhaging artery. You think your BP is ‘controlled’ if it’s 135/85? That’s still damage. And don’t get me started on Avastin being ‘just as good.’ It’s not. It’s cheaper. Big difference. The system doesn’t want you cured - it wants you returning monthly. 🤡
Divya Mallick
March 7, 2026 AT 14:59In India, we don’t have access to these fancy injections. My aunt got RVO. She went to a local clinic. They gave her steroids and told her to eat more turmeric. She lost 60% of her vision. Meanwhile, Americans whine about $50 vs $2000. This isn’t healthcare - it’s a luxury market. We need systemic change, not just better drugs. 🇮🇳✊
Pankaj Gupta
March 9, 2026 AT 05:26While the emotional weight of this condition is undeniable, it’s crucial to emphasize evidence-based interventions. Clinical trials consistently demonstrate that anti-VEGF therapy, regardless of brand, significantly reduces central retinal thickness and improves visual acuity. The key variable is adherence, not cost. Consistent follow-up with OCT imaging remains the gold standard. Precision matters.
Alex Brad
March 10, 2026 AT 12:06Avastin works. Get it. Don’t overthink it.
Renee Jackson
March 11, 2026 AT 05:01Thank you for this comprehensive, compassionate overview. It is imperative that patients understand that retinal vein occlusion is not merely an ocular event - it is a systemic sentinel. Proactive management of cardiovascular risk factors remains the cornerstone of long-term visual preservation. Consistency in treatment and lifestyle modification yields the most durable outcomes.
Richard Elric5111
March 12, 2026 AT 18:09One must contemplate the ontological paradox of medical intervention: if the body is a vessel of spirit, then to inject a protein inhibitor into the eye is to perform a ritual of control over nature’s equilibrium. Is healing the restoration of balance - or the imposition of pharmaceutical order? The retina, as the only window to the vascular system, becomes a canvas upon which modern medicine projects its hubris - and its hope.
Dean Jones
March 13, 2026 AT 04:20Look, I’ve been through this. Not just once - twice. First eye, then the other. The injections? Yeah, they’re annoying. The appointments? Exhausting. The fear? Real. But here’s what nobody tells you: the worst part isn’t the needle. It’s the silence afterward. The way your partner looks at you when you say, ‘I can’t read the clock.’ The way your kids stop asking you to help them with homework. The way you start avoiding mirrors. The drugs don’t fix that. They fix the swelling. But what fixes the loneliness? What fixes the grief? You don’t get a pamphlet for that. You just keep going. One injection at a time. Even when you’re tired. Even when you’re scared. Even when you don’t believe it’s worth it. You go. Because the alternative is worse. And if you’re lucky? One day, you’ll look up and realize you’ve been reading your grandkid’s drawings without even trying. That’s the win. Not the letters on the chart. The drawings.
Betsy Silverman
March 14, 2026 AT 04:39I’m a nurse who works in ophthalmology. I’ve seen hundreds of patients through this. The ones who survive - not just in vision, but in spirit - are the ones who have someone. A partner. A friend. A kid who texts them every day. Treatment isn’t just about the eye. It’s about connection. So if you’re reading this and you know someone going through this? Call them. Even if it’s just to say ‘Hey, how’s your week?’ That’s the real medicine.
Ivan Viktor
March 14, 2026 AT 14:55So let me get this straight. You’re telling me I need to get a needle shoved into my eyeball every month… for the rest of my life… because I didn’t quit smoking in 2008? Cool. Cool cool cool. 🤡 I’ll just go blind and call it a lifestyle choice.