

When someone has epilepsy, it means their brain has a tendency to produce sudden bursts of electrical activity that lead to seizures. Not every seizure means someone has epilepsy - you need at least two unprovoked seizures, or one seizure with a high chance of more, to be diagnosed. The epilepsy classification system used today was updated in January 2025 by the International League Against Epilepsy (ILAE), and it’s designed to help doctors choose the right treatment faster and avoid mistakes that can delay care.
How Seizures Are Classified Today
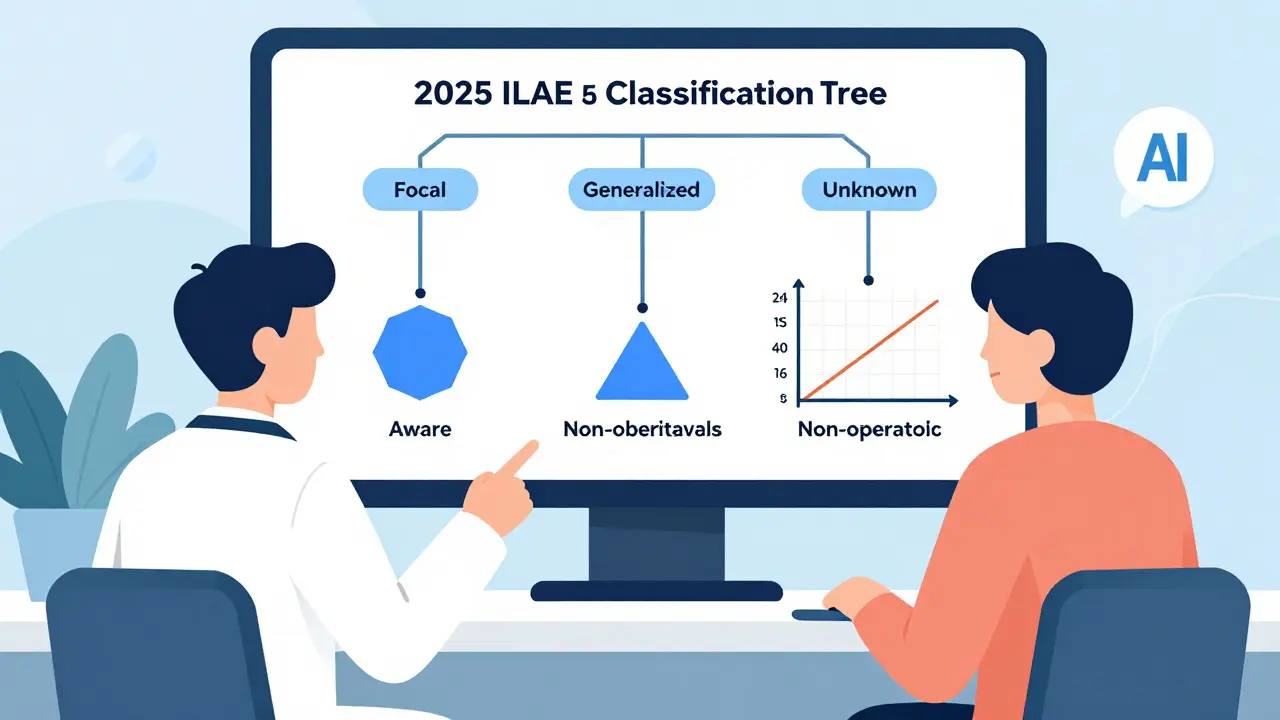
The old way of calling seizures "partial" or "complex" is gone. Now, seizures are grouped into four main types based on where they start in the brain:
- Focal seizures - start in one area of the brain. These make up about 60% of all epilepsy cases.
- Generalized seizures - involve both sides of the brain at once. These occur in about 30% of cases.
- Unknown onset - when there isn’t enough information to tell where the seizure began.
- Unclassified - rare cases where the seizure doesn’t fit any known pattern.
For focal seizures, doctors now use two key labels: aware (you stay awake and alert) and impaired awareness (you zone out or seem confused). About 25% of focal seizures are aware - meaning the person might feel a strange smell, see flashing lights, or get a rising feeling in their stomach. The other 75% are impaired awareness, where the person might stare blankly, fumble with clothes, or walk around without knowing it.
Generalized seizures come in six forms:
- Absence seizures - brief lapses in awareness, often mistaken for daydreaming. Common in children, making up 10-17% of childhood epilepsy.
- Myoclonic seizures - sudden muscle jerks, usually in the arms or shoulders.
- Tonic seizures - muscles stiffen, often causing falls.
- Clonic seizures - rhythmic jerking movements.
- Tonic-clonic seizures - the classic "grand mal" seizure: stiffening, shaking, loss of consciousness.
- Atonic seizures - muscles go limp, leading to sudden drops.
One big change in the 2025 update? They replaced "motor" and "non-motor" with "observable" and "non-observable." Why? Because some seizures don’t show outward signs - like a sudden feeling of fear, a strange taste, or a thought that feels foreign. These are just as real, just harder to spot.
What Causes Seizures to Happen
Triggers aren’t the same for everyone. Some people can go months without a seizure, then one event sets off a chain reaction. Common triggers include:
- Sleep deprivation - missing even one night of sleep can lower your seizure threshold.
- Stress - emotional or physical stress spikes cortisol, which can make the brain more excitable.
- Flashing lights - only affects about 3% of people with epilepsy, but it’s one of the most well-known triggers.
- Alcohol and withdrawal - drinking heavily or quitting cold turkey can trigger seizures within 6-48 hours.
- Missed medication - skipping even one dose increases seizure risk by 30% in some patients.
- Hormonal changes - many women with epilepsy have more seizures around their period, known as catamenial epilepsy.
- Infections or fever - especially in children or people with brain injuries.
But here’s the catch: not every seizure has a trigger. For many, seizures just happen. That’s why tracking them with a journal or app matters. A 2023 study of 850 patients found those who logged their seizures and possible triggers had 34% higher medication adherence and 41% fewer hospital visits.
How Antiepileptic Medications Work
There are over 30 FDA-approved antiepileptic drugs (AEDs), and no single one works for everyone. The goal isn’t to cure epilepsy - it’s to reduce or stop seizures with the fewest side effects.
Medications work in a few basic ways:
- Slowing down brain signals - drugs like levetiracetam and topiramate calm overactive nerve cells.
- Blocking sodium channels - carbamazepine, oxcarbazepine, and phenytoin stop the rapid firing of neurons.
- Boosting GABA - drugs like clonazepam and valproate increase the brain’s natural calming chemical.
Which drug you get depends on your seizure type:
- Focal seizures - lamotrigine, levetiracetam, lacosamide, and carbamazepine are first-line choices.
- Generalized seizures - valproate, ethosuximide (for absence), and lamotrigine are commonly used.
- Combined focal and generalized - valproate or lamotrigine are often chosen because they cover both types.
Side effects vary. Lamotrigine can cause a rare but serious skin rash. Valproate can affect liver function and is avoided in women of childbearing age due to birth defect risks. Levetiracetam may cause mood changes or irritability in about 10% of users.
Doctors don’t just pick a drug and hope for the best. They start low, go slow, and watch closely. It often takes 2-3 months to find the right dose. If one drug fails, they try another - and if two or three fail, they consider other options like surgery or nerve stimulation.
Why Misclassification Hurts
A 2023 study of 456 neurologists showed that using the old 2017 classification led to misdiagnosis in 32% of cases. The most common mix-up? Mistaking a focal seizure in the temporal lobe for a generalized seizure. Why does that matter?
If you have focal seizures but are treated like you have generalized epilepsy, you might get the wrong drug. For example, carbamazepine works well for focal seizures but can make some generalized seizures worse. One patient, diagnosed as having "generalized tonic-clonic seizures" for five years, later found out - after an EEG and detailed history - that her seizures started in one part of her brain. Switching to lacosamide stopped her seizures completely.
Even more troubling: 78% of patients in a 2023 survey said they were misdiagnosed at least once. The average time from first seizure to correct diagnosis? 2.3 years. That’s over two years of unnecessary fear, wrong meds, and missed work or school.
What’s New in 2025
The 2025 classification isn’t just a rename. It’s a smarter system. It reduced the number of named seizure types from 63 down to 21. Why? Because too many labels confused doctors and patients alike. Now, instead of memorizing dozens of rare terms, clinicians focus on the big picture: where did it start? Was awareness affected? What did it look like?
AI tools are coming. By late 2025, the ILAE will release a beta version of a digital assistant that helps non-specialists classify seizures using video clips and symptom descriptions. Early tests show it boosts accuracy by 18% for nurses and primary care doctors.
And the future? Genetic testing and brain biomarkers may soon become part of classification. By 2028, doctors might not just say "you have focal epilepsy" - they might say "you have SCN1A-related focal epilepsy," which tells them exactly which drugs to avoid and which to try.
What You Should Do
If you or someone you know has seizures:
- Get an EEG within 72 hours if possible - it’s the single most important test.
- Record seizures with video if you can - even a 10-second clip helps doctors see what’s happening.
- Keep a seizure diary - note time, duration, triggers, and how you felt before and after.
- Ask your doctor: "Is this focal or generalized? What type?" Don’t accept vague answers.
- If one medication doesn’t work after 3 months, don’t wait - ask about alternatives.
Accurate classification saves time, reduces side effects, and gets people back to living their lives. It’s not just medical jargon - it’s the difference between being stuck in a cycle of confusion and finding real control.
Can you have epilepsy without having convulsions?
Yes. Many people with epilepsy have seizures that don’t involve shaking or falling. Focal aware seizures might feel like a strange smell, sudden fear, or a buzzing sensation. Impaired awareness seizures can look like staring blankly, chewing without purpose, or walking around confused. These are just as real as convulsions and often get missed because they don’t look "dramatic."
Why do some people outgrow epilepsy?
Some epilepsy syndromes, like childhood absence epilepsy, are tied to brain development. As the brain matures, the abnormal electrical patterns fade. About 70% of children with absence seizures stop having them by age 18. But this doesn’t mean the brain is cured - it just means the specific wiring issue has resolved. Other types, especially those linked to brain injury or genetics, usually last a lifetime.
Are antiepileptic drugs addictive?
No, antiepileptic drugs are not addictive in the way opioids or benzodiazepines are. You don’t crave them or get high from them. But suddenly stopping them can trigger severe seizures or even a life-threatening condition called status epilepticus. That’s why doctors always taper them off slowly - not because they’re addictive, but because the brain needs time to adjust.
Can stress alone cause a seizure?
Stress doesn’t cause epilepsy, but it can trigger seizures in people who already have it. High stress raises cortisol and adrenaline, which can make the brain more likely to fire abnormally. For some, a single stressful event - like a breakup, job loss, or death in the family - can lead to multiple seizures over days or weeks. Managing stress through sleep, therapy, or mindfulness is often part of treatment.
Is epilepsy hereditary?
Some forms of epilepsy have strong genetic links - especially syndromes that start in childhood, like Dravet syndrome or juvenile myoclonic epilepsy. If a close family member has epilepsy, your risk is slightly higher, but most cases aren’t inherited. In fact, over half of people with epilepsy have no family history. Genetics plays a bigger role in certain types, but environment, injury, and infection matter just as much.
What Comes Next
For patients, the future is about precision. Instead of trying 3-4 drugs blindly, doctors will soon use genetic tests and brain scans to match treatments to individual biology. For the healthcare system, the challenge is making accurate classification accessible everywhere - not just in big hospitals, but in rural clinics and low-income countries where 75% of people with epilepsy still go undiagnosed.
One thing won’t change: epilepsy isn’t just about seizures. It’s about living fully - working, driving, parenting, traveling - without fear. And that starts with getting the diagnosis right the first time.
 Medications
Medications


Elaine Parra
March 25, 2026 AT 03:09And don't get me started on AI tools. You think a nurse in Kenya is gonna use some beta app to classify seizures? They're lucky if they have a flashlight that works.
Natasha Rodríguez Lara
March 25, 2026 AT 05:46Also, the part about non-observable seizures? My niece has them. She'll just freeze for 10 seconds, eyes glassy, no movement. Doctors used to think she was being defiant. Now we know. This matters.
peter vencken
March 25, 2026 AT 06:16also, levetiracetam wrecked my mood. like, full-on rage mode. switched to lacosamide. life changed. if u got mood issues, ask about that. not everyone gets the 'calm' meds.
Kevin Siewe
March 26, 2026 AT 09:12Also, the EEG within 72 hours advice? That’s gold. We waited 6 months. Don’t wait. Get it done. Even if it’s just a 20-minute routine EEG - it’s better than nothing.
Darlene Gomez
March 27, 2026 AT 04:37People with epilepsy aren’t broken. We’re not waiting to be 'cured.' We’re waiting for society to stop assuming we’re dangerous, unemployable, or incapable. My daughter has focal seizures. She’s a painter, a lifeguard, and she drives. She doesn’t need fixing. She needs access, accommodations, and less stigma.
Classifying seizures is useful. But let’s not forget the person behind the EEG.
Katie Putbrese
March 27, 2026 AT 06:07My cousin was misdiagnosed for years. They put her on valproate. She gained 70 pounds, lost her period, and still had seizures. Then she found a holistic doctor - no meds, just diet and magnesium. Zero seizures in 3 years.
Stop pushing drugs. Start pushing real healing.
Jacob Hessler
March 28, 2026 AT 16:44Blessing Ogboso
March 29, 2026 AT 08:28The new classification? It’s beautiful. But it’s meaningless if a child dies because no one knows how to recognize a myoclonic jerk.
What we need isn’t AI assistants - it’s training community health workers to spot seizures, to teach families what 'impaired awareness' looks like, to hand out one pill a day when they can’t afford ten.
Let’s not celebrate precision medicine while 75% of the world is still in the dark. The future of epilepsy care isn’t in labs - it’s in the hands of the village nurse who knows when to say, 'This is not normal.'