
Angina Treatment Selector
This tool helps identify the most appropriate angina treatment based on your symptoms, side effects, and medical conditions. Remember, this is for informational purposes only. Always discuss treatment options with your healthcare provider.
How can we help you?
Your Recommended Treatment
Key Considerations:
Important: This recommendation is based on general information provided in the article. Always consult with your doctor before making any changes to your medication regimen. Never stop or change your medication without medical supervision.
Quick Summary / Key Takeaways
- Nitroglycerin relieves angina quickly but can cause tolerance and headaches.
- Isosorbide dinitrate and isosorbide mononitrate give longer‑lasting relief with less rapid onset.
- Ranolazine works differently, targeting cellular metabolism rather than blood vessels.
- Beta‑blockers and calcium‑channel blockers address the root cause of chest pain by lowering heart workload.
- Choosing the right option depends on symptom pattern, co‑existing conditions, and lifestyle preferences.
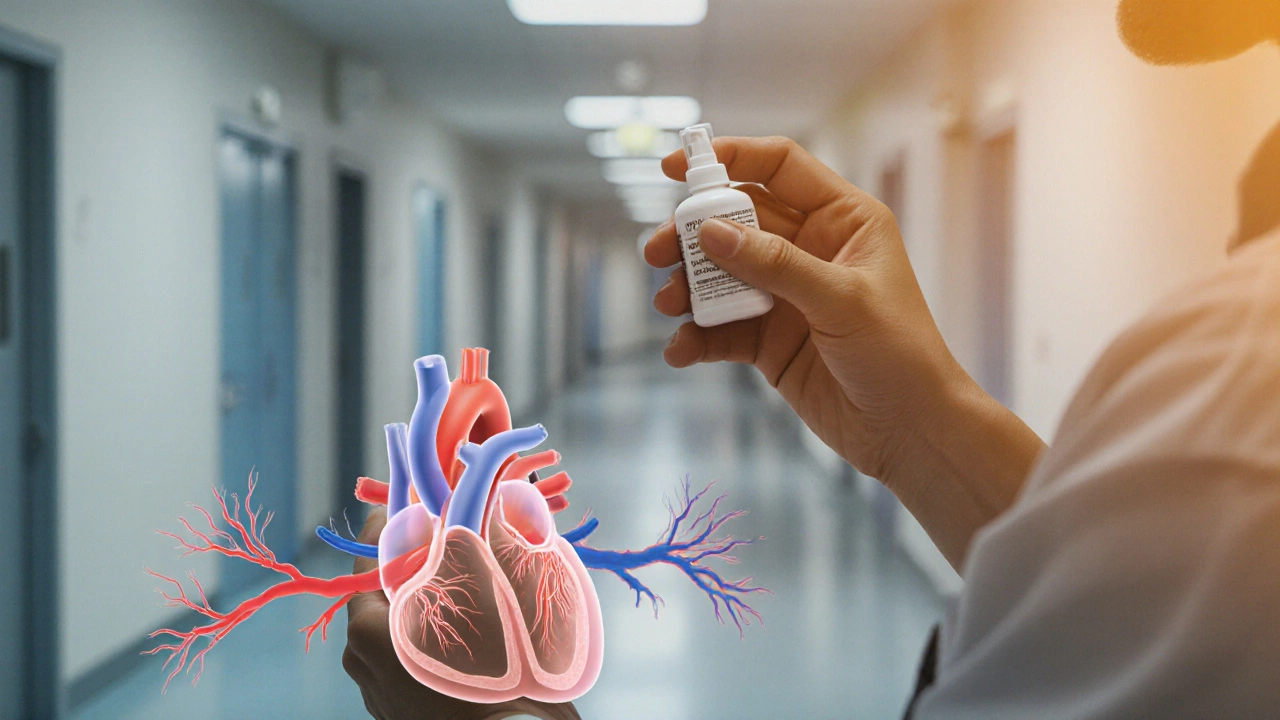
Understanding Nitroglycerin
Nitroglycerin is a fast‑acting nitrate medication that dilates coronary arteries and reduces cardiac preload, providing rapid relief for acute angina episodes. It comes as sublingual tablets, sprays, or transdermal patches. Onset is usually within 1‑3 minutes, and the effect lasts 15‑30 minutes. Because it releases nitric oxide directly, blood vessels relax, easing the heart’s oxygen demand.
While its speed is a huge advantage in emergencies, daily use often leads to nitrate tolerance - the drug becomes less effective after a few days. Common side effects include headache, flushing, and low blood pressure.
Why Look for Alternatives?
If you find yourself reaching for nitroglycerin multiple times a day, or if daily dosing triggers persistent headaches, it’s a sign that another strategy might work better. Alternatives can provide:
- Longer protection without the rapid‑onset headache spike.
- Simpler dosing schedules (once‑daily vs multiple daily doses).
- Different mechanisms that avoid nitrate tolerance altogether.
Most clinicians start with nitroglycerin for breakthrough pain, then add or switch to a longer‑acting agent for baseline control.
Top Alternatives Explained
Isosorbide Dinitrate
Isosorbide dinitrate is a organic nitrate that provides sustained vasodilation, typically taken 2‑3 times daily. It converts to nitric oxide slower than nitroglycerin, giving a smoother onset (5‑10 minutes) and lasting 4‑6 hours. Patients often experience fewer severe headaches because the plasma concentration rises more gradually.
Isosorbide Mononitrate
Isosorbide mononitrate is a single‑dose nitrate that offers 24‑hour coverage with once‑daily dosing. It does not need metabolic activation, which makes its effect more predictable. Side‑effects are similar to dinitrate but generally milder.
Ranolazine
Ranolazine is a p‑type anti‑anginal agent that improves myocardial efficiency by shifting cardiac metabolism from fatty acids to glucose. Unlike nitrates, it does not cause vasodilation, so dizziness and headaches are rare. Typical dosing starts at 500mg twice daily, titrating to 1000mg twice daily. Onset is slower (several days) but provides steady symptom control.
Beta‑Blockers (example: Metoprolol)
Metoprolol is a cardioselective beta‑1 blocker that lowers heart rate and contractility, reducing oxygen demand. It’s useful for patients whose angina is triggered by exertion or stress. Doses range from 25mg to 200mg daily, often split into two doses. Side‑effects can include fatigue, cold hands, and mild depression.
Calcium‑Channel Blockers (example: Amlodipine)
Amlodipine is a dihydropyridine calcium‑channel blocker that relaxes arterial smooth muscle, improving coronary blood flow. It works well for patients with hypertension‑related angina. Typical dose is 5‑10mg once daily. Common complaints are ankle swelling and a slight flushing sensation.
Side‑by‑Side Comparison
| Drug | Mechanism | Typical Dose | Onset | Duration | Pros | Cons |
|---|---|---|---|---|---|---|
| Nitroglycerin | Rapid nitric‑oxide release → vasodilation | 0.3‑0.6mg sublingual; 0.2‑0.4mg spray | 1‑3min | 15‑30min | Fast relief, easy rescue use | Headache, tolerance, short‑acting |
| Isosorbide dinitrate | Slow‑release nitrate → sustained vasodilation | 5‑10mg 2‑3×/day | 5‑10min | 4‑6hr | Longer coverage, fewer spikes | Requires dosing schedule, still tolerance |
| Isosorbide mononitrate | Single‑dose nitrate → steady plasma level | 20‑40mg once daily | 30‑60min | 24hr | Once‑daily convenience | May still cause headache, not immediate relief |
| Ranolazine | Metabolic shift → improved efficiency | 500‑1000mg BID | Days to steady state | 24hr | No vasodilation side‑effects | Cost, possible QT prolongation |
| Metoprolol (β‑blocker) | β‑1 blockade → lower heart rate & contractility | 25‑200mg daily (often split) | 30‑60min | 12‑24hr | Addresses trigger, improves survival | Fatigue, bronchospasm risk |
| Amlodipine (CCB) | Calcium‑channel inhibition → arterial dilation | 5‑10mg daily | 30‑60min | 24hr | Effective for hypertensive angina | Edema, gum hyperplasia |
Choosing the Right Option for You
Start by answering three personal questions:
- Do you need **instant** relief (e.g., unpredictable chest pain) or steady‑state control?
- Are headaches or low blood pressure limiting your current nitroglycerin use?
- Do you have other conditions-high blood pressure, asthma, or heart failure-that influence drug choice?
If the answer to #1 is “yes,” keep nitroglycerin as a rescue pill but add a long‑acting nitrate or a non‑nitrate agent for background protection. If #2 is “yes,” switch to isosorbide mononitrate or a beta‑blocker, which usually cause fewer headaches. If #3 is “yes,” a calcium‑channel blocker may handle both hypertension and angina, while ranolazine can be a safe third‑line option if you’re already on a beta‑blocker and a nitrate.
Always discuss with your cardiologist before swapping drugs. They’ll check for interactions-especially between nitrates and phosphodiesterase‑5 inhibitors (like Viagra), which can cause dangerous drops in blood pressure.
Practical Tips to Minimize Side Effects
- Schedule a daily nitrate‑free interval (usually overnight) to reset tolerance.
- Take nitroglycerin with a glass of water, avoid crushing tablets unless prescribed.
- Start beta‑blockers at low dose; increase gradually to avoid sudden heart‑rate drops.
- Monitor blood pressure weekly when you add a calcium‑channel blocker.
- Report any persistent dizziness, palpitations, or unusual fatigue to your doctor promptly.
Frequently Asked Questions
Can I use nitroglycerin and a beta‑blocker together?
Yes, they work via different pathways-nitroglycerin for quick relief and beta‑blockers for long‑term heart‑rate control. However, monitor for low blood pressure and discuss dosage timing with your doctor.
Why do I still get headaches on isosorbide mononitrate?
Headaches stem from vasodilation of cranial vessels. If they persist, your doctor might lower the dose, split it into twice‑daily dosing, or switch to a non‑nitrate such as ranolazine.
Is ranolazine safe for people with kidney problems?
Ranolazine is cleared partly by kidneys. For severe renal impairment (eGFR <30ml/min), dosage reduction or avoidance is recommended. Always get baseline labs before starting.
Do calcium‑channel blockers interact with nitroglycerin?
There is no major pharmacokinetic interaction, but both cause vasodilation, so combined use may increase the risk of low blood pressure. Your clinician may adjust doses accordingly.
How long does nitrate tolerance take to develop?
Tolerance can appear after 24‑48hours of continuous exposure. A nightly nitrate‑free interval of 8‑12hours usually restores full responsiveness.
 Medications
Medications


RaeLyn Boothe
October 11, 2025 AT 23:58If you keep reaching for nitroglycerin five times a day, you’re basically flirting with tolerance, and the headaches become a daily alarm clock.
Fatima Sami
October 12, 2025 AT 02:11The article mistakenly uses “dinitrate” where “mononitrate” is meant. Also, the phrase “the it” appears in a sentence; it should be removed.
Stephanie Jones
October 12, 2025 AT 04:24When we talk about nitroglycerin we are really discussing a fleeting promise, a chemical whisper that tells the heart to pause its frantic race, only to remind us that relief is as fragile as a sigh in a storm.
Nathan Hamer
October 12, 2025 AT 06:38Ah, the dance of nitrates and the human heart is nothing short of a tragic opera!
Every sublingual tablet delivers a fleeting surge of nitric oxide, like a bolt of lightning striking a storm‑tossed sea.
The immediate relief is intoxicating, yet the price is paid in throbbing temples that echo the very pressure the drug was meant to alleviate.
Your body, wise as it is, learns to ignore the message after a handful of doses, a phenomenon we call tolerance.
When tolerance sets in, the same mg no longer opens the coronary vessels, leaving you pleading for the next hit.
Enter the nitrate‑free interval, the nocturnal pause that resets the system, but most patients forget to schedule it.
Alternatives like isosorbide mononitrate replace the flash with a steady glow, smoothing out the peaks and valleys of angina.
Ranolazine, on the other hand, sidesteps the vasodilatory pathway entirely, coaxing the myocardium to sip fuel more efficiently.
Beta‑blockers temper the heart’s frantic beating, reducing oxygen demand without widening the blood vessels.
Calcium‑channel blockers, such as amlodipine, widen the arterial highways, delivering blood to the starving myocardium.
Each class carries its own side‑effect constellation; headaches for nitrates, edema for amlodipine, fatigue for betas.
Choosing the right hero depends on your personal saga-whether you crave instant rescue or a chronic shield.
Never pair nitrates with phosphodiesterase‑5 inhibitors; the combination can plunge you into a black‑out of blood pressure.
Regular follow‑ups with your cardiologist are essential, as dosage tweaks can turn a nightmare into a manageable routine.
In short, respect the power of nitroglycerin, honor its limits, and let the alternatives fill the gaps where it falters. 🌟💊
Tom Smith
October 12, 2025 AT 08:51So you’ve mastered the art of copying a Wikipedia page and pasted it here-bravo! If you want a real discussion, try adding a source that isn’t a broken link, then maybe we’ll pretend to care.
Kyah Chan
October 12, 2025 AT 11:04The presentation suffers from a lack of coherent structure; headings are interspersed with raw JavaScript, impairing readability. Moreover, the table lacks proper captioning, which contravenes accessibility standards.
Ira Andani Agustianingrum
October 12, 2025 AT 13:18Hey folks, just a heads‑up: if you’re dealing with nitroglycerin headaches, try taking the dose with a full glass of water and stay upright for a few minutes. Also, keep a log of when you use it-your doc will love the data.
James Higdon
October 12, 2025 AT 15:31From an ethical standpoint, it is incumbent upon healthcare providers to ensure patients are fully informed about the risk of nitrate tolerance before prescribing chronic nitroglycerin therapy.
Wanda Smith
October 12, 2025 AT 17:44The conspiratorial narrative woven around pharmaceutical giants suggests that the true purpose of nitrate drugs is to keep us dependent on perpetual pain relief, a subtle form of control masked as care.
Bridget Jonesberg
October 12, 2025 AT 19:58While the preceding comment delves into the nebulous realm of alleged corporate machinations, it is essential to juxtapose such speculation with empirical evidence, lest we descend into mere hyperbole; indeed, the pharmacokinetic profile of nitroglycerin, characterized by rapid hepatic first‑pass metabolism, underscores its suitability for episodic deployment, yet simultaneously begets the phenomenon of tachyphylaxis, thereby necessitating judicious scheduling of nitrate‑free intervals to preclude desensitization-a nuance often obfuscated in lay discussions.
Marvin Powers
October 12, 2025 AT 22:11Let’s talk culture, shall we? In some parts of the world, nitroglycerin is hailed as the hero, while in others it’s the villain-so much for a universal standard! The irony is that doctors love their fancy acronyms, but patients just want relief without the migraine side‑effects. Spoiler: you can mix a beta‑blocker with a calcium‑channel blocker, and it works perfectly-unless you’re on a PDE‑5 inhibitor, then you’ll be floating. Remember, the guidelines are written by committees that love footnotes, not by the guy in the ER who gave you that sublingual spray. So, next time you’re on a nitro‑free day, enjoy the calm before the storm; it’s called a “nitrate holiday.”
Jaime Torres
October 13, 2025 AT 00:24Nitrates work quick.
Wayne Adler
October 13, 2025 AT 02:38Listen, the whole deal with nitrates is you cant keep taking them nonstop, your body just learns to ignore them and then you're stuck with chest pain again-so you gotta plan those nitrate‑free windows. If u dont do it, u end up with tolerance faster than a meme goes viral.
Shane Hall
October 13, 2025 AT 04:51Here’s the playbook: start with acute nitroglycerin for those sudden attacks, then transition to a long‑acting nitrate like isosorbide mononitrate for baseline control, and if headaches persist, consider swapping to ranolazine or a beta‑blocker. Keep a symptom diary, talk to your cardiologist about dosage tweaks, and never, ever combine nitrates with Viagra. This systematic approach will keep your heart beating in rhythm without the unwanted side‑effects.
Christopher Montenegro
October 13, 2025 AT 07:04From a pharmacodynamic perspective, the rapid vasodilatory cascade induced by nitroglycerin via nitric oxide liberation entails a transient reduction in preload, yet the concomitant reflex tachycardia may offset myocardial oxygen consumption; therefore, a nuanced therapeutic algorithm incorporating pharmacokinetic profiling and patient‑specific comorbidities is mandatory to mitigate adverse events and optimize hemodynamic stability.